Paramedic OSCE scenarios test your ability to assess, treat, and communicate under pressure. Every university structures their OSCE differently, but the scenario categories are remarkably consistent. If you can handle each of these categories systematically, you can handle whatever station they put in front of you.
This guide breaks down each scenario category, what examiners are looking for, and how to approach them. Use it alongside AI OSCE practice to drill scenarios across every category.
Cardiac Scenarios
Cardiac presentations are the bread and butter of paramedic OSCEs. They test your ability to recognise time-critical conditions and act decisively.
Common scenarios: ACS/STEMI, atrial fibrillation, cardiac arrest, bradycardia, SVT, heart failure.
What examiners expect:
- Systematic ABCDE assessment with early focus on circulation
- 12-lead ECG interpretation (or at minimum, recognising the need for one)
- SOCRATES pain assessment for chest pain presentations
- Knowledge of time-critical pathways (PPCI for STEMI, stroke pathway for AF with neurological symptoms)
- Appropriate pharmacology — GTN, aspirin, morphine — with contraindication checks
- Recognition of deterioration and escalation
Common mistakes: Jumping straight to "it's an MI" without completing a systematic assessment. Forgetting to check allergies before administering aspirin. Not considering differentials — chest pain has many causes beyond ACS.
Approach tip: For any chest pain scenario, always run through your differentials aloud: cardiac, respiratory (PE, pneumothorax), musculoskeletal, GI (reflux). Even if your working diagnosis is ACS, showing you've considered alternatives demonstrates clinical reasoning.
Respiratory Scenarios
Respiratory emergencies require rapid assessment and confident intervention. These scenarios test whether you can identify the severity of a respiratory condition and act appropriately.
Common scenarios: Acute asthma, COPD exacerbation, pneumonia, anaphylaxis, tension pneumothorax.
What examiners expect:
- Airway assessment before anything else
- Accurate respiratory rate, SpO2, and work of breathing assessment
- Correct oxygen therapy — knowing when to use high-flow vs controlled oxygen (particularly important for COPD)
- Inhaler/nebuliser technique and drug knowledge
- Recognition of life-threatening features (silent chest in asthma, see-saw breathing)
- Peak flow measurement where appropriate
Common mistakes: Defaulting to high-flow oxygen for every patient. Not recognising the difference between moderate, severe, and life-threatening asthma. Forgetting to reassess after treatment.
Approach tip: For respiratory scenarios, always state the respiratory rate, oxygen saturations, and work of breathing explicitly. These are your three key observations. If you cannot find them all, say so — "I would like to check the SpO2 but the patient's fingers are cold" shows the examiner you know what you're looking for.
Neurological Scenarios
Neurological assessments can feel overwhelming, but they follow the same ABCDE framework as everything else. The key difference is the focus on Disability (the D in ABCDE).
Common scenarios: Stroke (FAST positive), head injury, seizure, hypoglycaemia, altered consciousness.
What examiners expect:
- GCS assessment with correct scoring across eye, verbal, and motor responses
- FAST assessment for suspected stroke
- Blood glucose measurement — this should be almost automatic for any altered consciousness
- Pupil assessment (PEARL — Pupils Equal And Reactive to Light)
- Knowledge of time-critical pathways (stroke pathway, head injury criteria)
- Cervical spine consideration in trauma-related neurological presentations
Common mistakes: Forgetting to check blood glucose. Saying "GCS is 12" without breaking it down into E3 V4 M5 (or whatever the components are). Not assessing pupils. Assuming altered consciousness is always neurological — consider metabolic, toxicological, and traumatic causes.
Approach tip: For any patient with altered consciousness, your first three actions after ABCDE primary survey should be: blood glucose, pupil assessment, GCS. State these clearly. If the blood glucose is low, treat it immediately — this is a reversible cause and treating it early can change the entire clinical picture.
Trauma Scenarios
Trauma OSCEs test your ability to manage potentially life-threatening injuries systematically while maintaining c-spine awareness throughout.
Common scenarios: RTC with multiple injuries, falls in elderly patients, penetrating trauma, burns, limb injuries.
What examiners expect:
- C-spine awareness from the moment you approach the patient
- Catastrophic haemorrhage control (cABCDE — the c comes first in trauma)
- Systematic head-to-toe secondary survey
- Appropriate splinting and immobilisation decisions
- Burns assessment using Wallace Rule of Nines
- Trauma-specific handover (ATMIST format)
- Recognition of internal bleeding signs
Common mistakes: Forgetting c-spine considerations. Not controlling visible haemorrhage before moving to airway. Poor burns percentage estimation. Spending too long on the secondary survey and running out of time for treatment and handover.
Approach tip: In trauma, remember cABCDE — catastrophic haemorrhage comes first. State "checking for catastrophic haemorrhage" as your first action after scene safety. This alone can pick up marks that many students miss.
Paediatric Scenarios
Paediatric presentations make students nervous, but the approach is fundamentally the same as adult assessment with age-appropriate modifications.
Common scenarios: Febrile convulsion, croup, bronchiolitis, paediatric sepsis, non-accidental injury assessment.
What examiners expect:
- Age-appropriate communication (talking to both the child and the parent/carer)
- Correct paediatric vital sign ranges for the child's age
- Weight-based drug dosing awareness
- Recognition of the seriously unwell child (traffic light system)
- Safeguarding awareness — asking appropriate questions if non-accidental injury is a concern
- Appropriate escalation and transport decisions
Common mistakes: Ignoring the parent — they are your best source of history. Using adult normal ranges for paediatric vital signs. Not adapting communication style to the child's developmental stage. Being afraid to mention safeguarding concerns.
Approach tip: Always involve the parent/carer in your assessment. "Can you tell me what happened?" directed at the parent is often more productive than trying to get a history from a distressed 3-year-old. But do engage with the child — introduce yourself at their level, use their name, and explain things simply.
Communication Scenarios
Communication stations explicitly test your interpersonal skills. These may involve structured handovers, breaking bad news, managing conflict, or dealing with capacity issues.
Common scenarios: SBAR/ATMIST handover to hospital, breaking bad news, managing an angry relative, mental capacity assessment, obtaining informed consent.
What examiners expect:
- Structured handover using SBAR or ATMIST (know which your university prefers)
- Active listening — letting the patient or relative speak without interrupting
- Empathy and compassion — acknowledging emotions before giving information
- Clear, jargon-free language when explaining to patients
- Knowledge of Mental Capacity Act principles
- Professional boundary awareness
Common mistakes: Rushing the handover and missing key information. Using medical jargon with patients. Not pausing to acknowledge the patient's emotional state. Giving too much information at once.
Approach tip: For handover stations, practise delivering a complete ATMIST or SBAR in under 60 seconds. Time yourself. The structure should be so automatic that you can deliver it under pressure without thinking about the format — all your cognitive effort should be on the clinical content.
Mental Health Scenarios
Mental health OSCE stations assess your ability to perform compassionate, structured assessments in sensitive situations.
Common scenarios: Self-harm assessment, suicidal ideation, acute psychosis, substance misuse, section 136 assessment.
What examiners expect:
- Non-judgemental approach and language
- Direct questions about self-harm and suicidal intent (asking directly does not increase risk)
- Structured risk assessment
- Knowledge of relevant legislation (Mental Health Act, Mental Capacity Act)
- Appropriate safety planning and referral
- Scene and personal safety awareness
Common mistakes: Avoiding direct questions about suicide — "Have you thought about harming yourself?" is a necessary question, not a harmful one. Being visibly uncomfortable, which transfers to the patient. Forgetting physical health assessment — mental health presentations can have physical causes.
Approach tip: Mental health scenarios reward calmness and empathy above all else. Sit at the patient's level, maintain appropriate eye contact, and use open questions. "Can you tell me what's been happening for you recently?" opens far more than "Are you suicidal?" as a first question. Build rapport before asking the more direct risk assessment questions.
How to Use This Guide
- Read through each category and identify where you feel least confident. That's where you should focus your practice
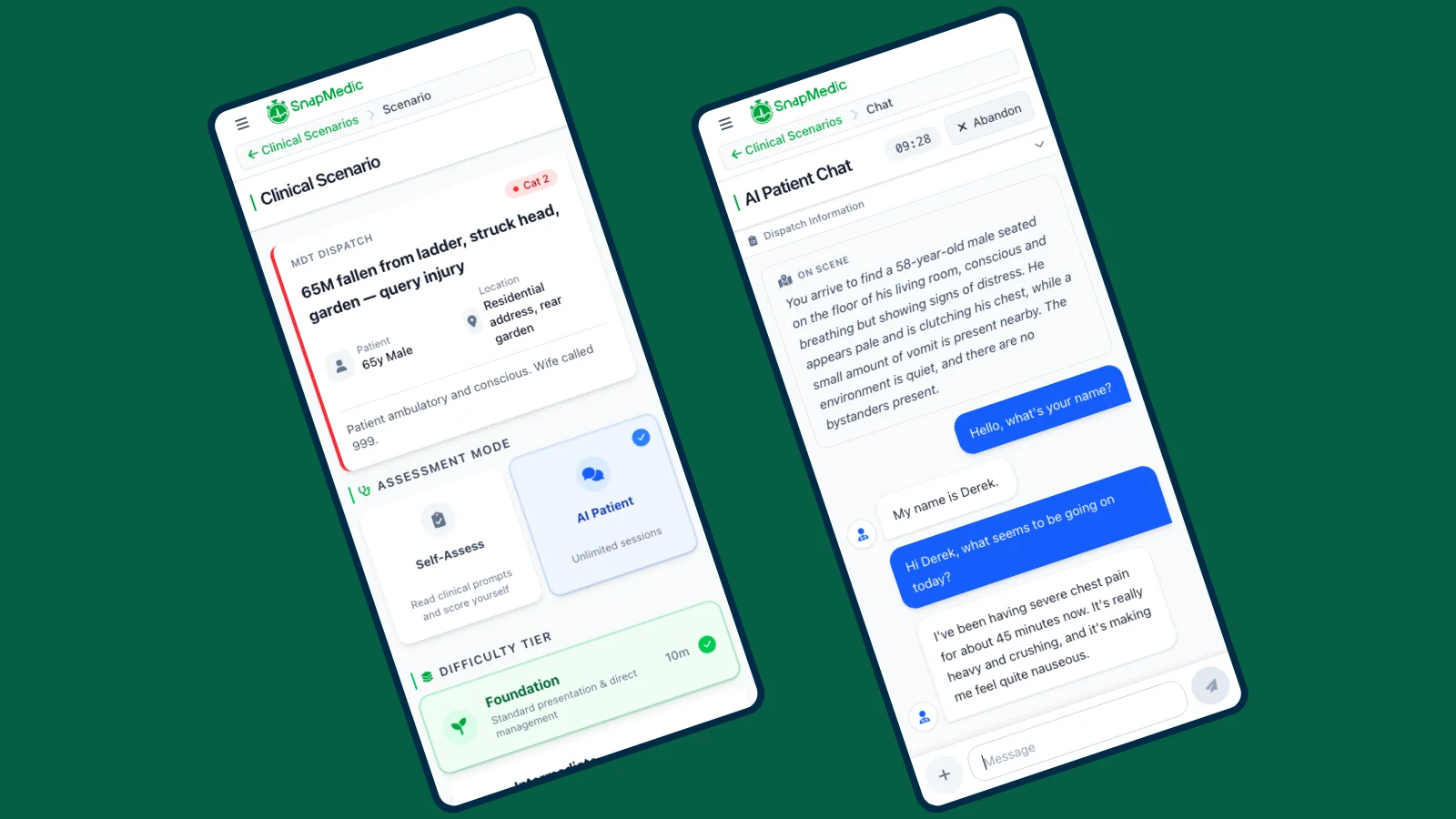
- Use AI OSCE Practice to run scenarios in your weak areas. SnapMedic covers all the categories above at Foundation, Intermediate, and Advanced difficulty
- Time yourself during practice. If you consistently run out of time, you're spending too long on one section
- Review your feedback after each AI session. The structured marking highlights exactly where you lost points
- Repeat — run the same category multiple times until your approach is automatic, then move on
For a broader overview of OSCE preparation strategy, read our guide on how to pass your paramedic OSCE.
Download SnapMedic
AI-powered OSCE practice across every scenario category — built for UK paramedics
Or try the web version
Free to download • All core features included • Works offline